
If you’ve been offered a free hearing test at a shopping centre kiosk or been told your entire hearing assessment will take “just 20 minutes,” you might be wondering whether that’s really sufficient. The short answer? It’s not. A proper, comprehensive hearing assessment requires substantially more time—typically between 60 and 90 minutes—and involves multiple test components that simply cannot be adequately performed in a rushed appointment.
Understanding what should be included in a thorough audiological assessment is essential, not just for your hearing health, but for ensuring any subsequent recommendations for hearing aids or other interventions are based on accurate, complete information. Let’s explore why a quick hearing test falls short, what you should expect from a comprehensive assessment, and when you need to question whether you’ve received adequate testing.
What Actually Happens During a Comprehensive Hearing Assessment?
A properly conducted hearing test isn’t a single examination—it’s a series of carefully sequenced assessments that together paint a complete picture of your auditory system. According to Audiology Australia’s professional practice standards and international protocols from bodies such as the British Society of Audiology, a diagnostic hearing assessment should include the following components.
Case History (10–15 Minutes)
Your audiologist should begin by gathering detailed information about your hearing concerns, medical history, noise exposure, family history of hearing loss, medications, and the specific situations where you struggle to hear. This conversation isn’t mere box-ticking; it directly informs which tests are prioritised and helps establish whether your hearing difficulties might stem from medical conditions requiring referral to an ear, nose and throat specialist.
A rushed case history means critical information may be missed—perhaps a recent head injury, sudden hearing changes, or dizziness that could indicate more serious underlying pathology. This initial conversation establishes the foundation for everything that follows.
Otoscopy (2–3 Minutes)
Before placing anything in your ears, your audiologist should examine your ear canals and eardrums using an otoscope. This visual inspection identifies wax occlusion, foreign bodies, perforations, infections, or abnormalities that could affect test results or require medical attention before proceeding.
A 20-minute hearing test often skips thorough otoscopy or performs it cursorily, potentially missing conditions that invalidate the subsequent results or require medical intervention.
Tympanometry and Middle Ear Function (5 Minutes)
Tympanometry measures how your eardrum moves in response to air pressure changes, assessing middle ear function. This objective test identifies fluid behind the eardrum, Eustachian tube dysfunction, ossicular chain problems, or eardrum perforations—all conditions that affect hearing but won’t necessarily show up clearly on a basic hearing threshold test.
Combined with acoustic reflex testing (discussed below), tympanometry provides crucial diagnostic information that helps differentiate between conductive hearing loss (middle ear problems, often medically treatable) and sensorineural hearing loss (inner ear or nerve-related). Quick hearing tests frequently omit this entirely, potentially missing treatable medical conditions.
Pure Tone Audiometry: Air Conduction (15–20 Minutes)
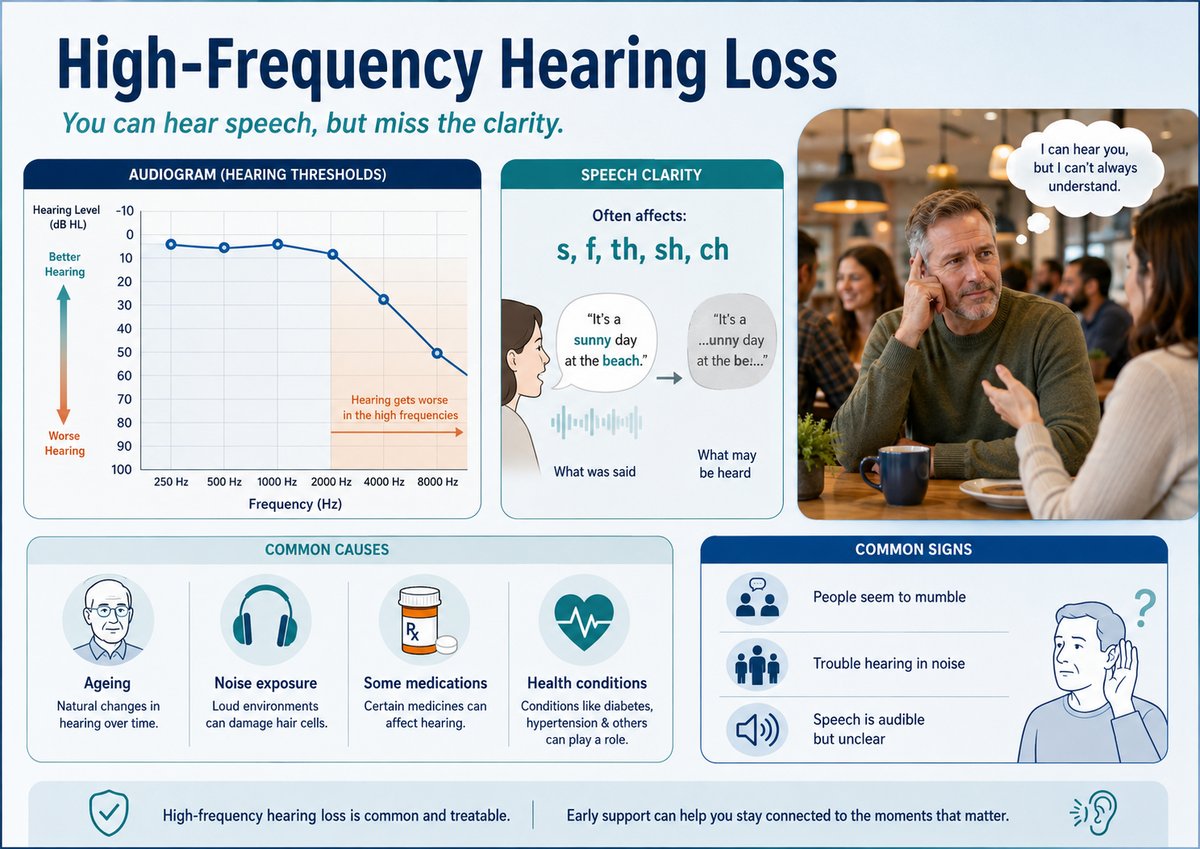
This is the test most people associate with hearing assessments—wearing headphones and pressing a button when you hear beeps at different pitches and volumes. However, thorough air conduction testing should assess frequencies from 250 Hz through to 8000 Hz at minimum, with some protocols extending to 12,000 Hz or 16,000 Hz to detect early noise-induced hearing loss or ototoxicity.
Each ear requires individual testing across all frequencies, with careful threshold determination using proper clinical technique. Rushing this process or testing limited frequencies produces incomplete data that might miss crucial patterns—such as high-frequency loss affecting speech clarity or asymmetrical hearing loss warranting medical investigation.
Pure Tone Audiometry: Bone Conduction (5–10 Minutes)
Bone conduction testing uses a vibrating device placed on the mastoid bone behind your ear, bypassing the outer and middle ear to test inner ear function directly. By comparing air conduction and bone conduction results, audiologists can definitively identify whether hearing loss originates from the middle ear (conductive loss, often medically treatable) or the inner ear (sensorineural loss).
This component is frequently eliminated from short hearing tests, despite being clinically essential for proper diagnosis and referral decisions. Without bone conduction testing, you’re left with an incomplete picture that could delay appropriate medical treatment.
Speech Testing in Quiet (5 Minutes)
Understanding speech is fundamentally different from detecting pure tones. Speech audiometry in quiet conditions establishes your speech recognition threshold (the softest level at which you can repeat back words) and word recognition score (how accurately you identify words at comfortable listening levels).
These measures validate pure tone results and provide functional information about real-world communication abilities. They’re particularly important for predicting hearing aid benefit and establishing baseline performance.
Speech Testing in Noise (10 Minutes)
Here’s where comprehensive testing diverges dramatically from quick assessments. Speech-in-noise testing evaluates how well you understand speech when competing background noise is present—the exact situation where most people with hearing loss struggle most.
Tests such as the QuickSIN (Quick Speech-in-Noise) or the Australian-developed BKB-SIN assess your signal-to-noise ratio loss, quantifying how much louder speech needs to be relative to background noise for you to understand it. This information is invaluable for:
– Determining candidacy for directional microphones and advanced noise reduction features
– Setting realistic expectations about hearing aid performance in challenging environments
– Identifying auditory processing difficulties that might require different management approaches
– Establishing baseline performance for measuring rehabilitation outcomes
The 20-minute hearing test almost universally omits speech-in-noise assessment, despite it being the most functionally relevant test for most patients. This omission means recommendations are based on incomplete data that doesn’t reflect your actual communication challenges.
Acoustic Reflex Testing (5 Minutes)
Acoustic reflex measurements detect the contraction of middle ear muscles in response to loud sounds. These objective tests (you don’t need to respond—the equipment measures the physiological response) provide diagnostic information about:
– Facial nerve function
– Auditory nerve integrity
– Brainstem auditory pathway function
– Severity and type of hearing loss
– Retrocochlear pathology that might indicate acoustic neuroma or other conditions requiring urgent medical referral
Quick hearing tests routinely skip acoustic reflexes, potentially missing red flags that warrant immediate specialist referral.
Explanation of Results and Recommendations (10–15 Minutes)
A comprehensive assessment concludes with your audiologist explaining what the tests revealed, what it means for your hearing health, and what options are available. This discussion should cover:
– The type, degree, and configuration of any hearing loss
– Likely causes and whether medical referral is indicated
– How your hearing loss affects communication in various environments
– Evidence-based management options, which might include hearing aids, assistive listening devices, communication strategies, or simply monitoring
– Realistic expectations about outcomes
– Follow-up plans
Adequate time for questions and genuine understanding is essential. A rushed explanation leaves patients confused about their results and unprepared to make informed decisions about management.
What You Miss with Quick Hearing Tests
When an assessment is compressed into 20 minutes, significant compromises occur. Typically, these abbreviated tests include only:
– Cursory case history
– Basic otoscopy (sometimes)
– Air conduction pure tone audiometry, often at limited frequencies
– Brief explanation focused primarily on selling hearing aids
The following critical components are usually omitted:
– Tympanometry and middle ear assessment
– Bone conduction testing
– Speech-in-noise evaluation
– Acoustic reflex testing
– Extended high-frequency testing
– Thorough explanation of results
– Consideration of non-hearing-aid management options
This isn’t merely about thoroughness for thoroughness’s sake. These omissions have real clinical consequences. Without complete diagnostic information, you might:
– Miss medically treatable conditions requiring specialist referral
– Receive inappropriate or premature hearing aid recommendations
– Purchase hearing aids not optimally programmed for your specific hearing loss configuration
– Lack baseline measurements needed to track progression or rehabilitation outcomes
– Remain unaware of auditory processing difficulties or other complicating factors
Furthermore, abbreviated testing in retail environments often serves primarily as a sales tool rather than a comprehensive diagnostic assessment. The pressure to sell hearing aids can compromise clinical objectivity, and the limited data gathered may not support evidence-based decision-making.
When Should You Question Your Hearing Test?
Not every situation requires the full 90-minute assessment described above. Routine monitoring appointments for stable hearing loss, for instance, might appropriately take less time. However, you should question the adequacy of your testing if:
– You’re a new patient and the entire appointment, including discussion, takes less than 45 minutes
– You’ve never had tympanometry or bone conduction testing performed
– You’ve never been assessed for speech understanding in background noise
– Your audiologist can’t show you a complete audiogram with both air and bone conduction results
– You receive hearing aid recommendations without thorough testing or discussion of your specific communication needs
– You experience dizziness, sudden hearing changes, or one-sided hearing loss but weren’t referred for medical evaluation
– The appointment felt rushed, your questions weren’t adequately answered, or you left feeling uncertain about your results
What to Expect from Proper Comprehensive Testing
When you attend a thorough audiological assessment, you should experience:
A collaborative, unhurried process where you feel heard and your concerns are taken seriously, with adequate time for all test components and discussion.
Multiple different tests using various equipment and techniques, not just the basic headphone beep test.
Clear explanations of what each test measures, why it’s being performed, and what the results mean in practical terms for your daily communication.
A complete audiogram showing both air and bone conduction results across all relevant frequencies, with speech testing results and middle ear measurements documented.
Honest, balanced advice about all management options, including situations where hearing aids might not be the first recommendation or where medical referral takes priority.
Written documentation of your results, recommendations, and follow-up plans that you can take home and review.
Time for questions without feeling rushed or pressured toward a particular decision.
According to Audiology Australia’s professional practice guidelines, comprehensive diagnostic assessment forms the foundation of evidence-based audiological care. Shortcuts in testing undermine clinical quality and patient outcomes.
Making Informed Decisions About Your Hearing Health
Your hearing is too important to trust to incomplete assessment. While free or quick hearing tests might seem convenient, they rarely provide the comprehensive information necessary for accurate diagnosis and optimal management recommendations.
If you’re concerned about your hearing, seek out a qualified audiologist who conducts thorough assessments following best practice protocols. Ask how long the appointment will take and what tests will be included. A comprehensive initial assessment typically requires 60–90 minutes, and this time investment pays dividends in accurate diagnosis, appropriate recommendations, and better long-term outcomes.
Remember, a hearing assessment should be a diagnostic health appointment, not a sales interaction. You deserve complete, accurate information about your hearing health, delivered by a professional who prioritises clinical best practice over commercial pressure.




{kind=link}
{kind=link}
{kind=link}