
When you’re told you have hearing loss, one of the first questions your audiologist will answer is *what type* of hearing loss you have. This distinction matters enormously—not just for understanding what’s happened to your hearing, but for determining whether your hearing loss can be reversed, managed, or requires specialist medical intervention.
The two main categories—conductive and sensorineural hearing loss—may sound like technical jargon, but they describe fundamentally different problems occurring in different parts of your auditory system. Understanding the difference between conductive and sensorineural hearing loss is essential for anyone navigating a new diagnosis, supporting a family member, or simply trying to make sense of their audiogram results.
In this article, we’ll break down these types of hearing loss in plain English, explain how audiologists differentiate between them, and outline what each diagnosis means for your treatment options.
Understanding the Auditory System: A Quick Anatomy Lesson
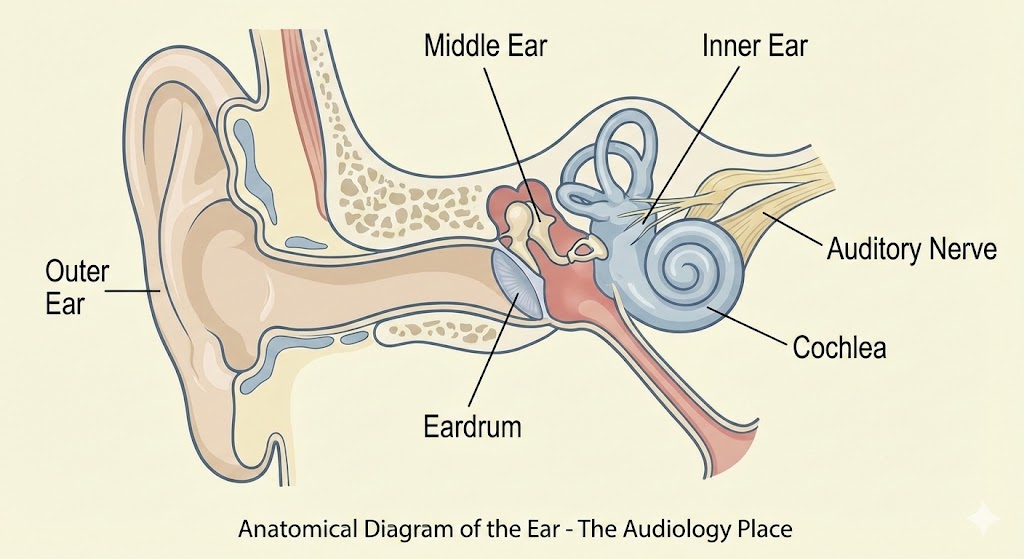
Before we dive into the differences, it helps to understand the basic architecture of your hearing system. Your ear is divided into three main sections:
– Outer ear: The visible part (pinna) and the ear canal leading to the eardrum
– Middle ear: The air-filled space containing three tiny bones (ossicles) that amplify sound vibrations
– Inner ear: The cochlea, a snail-shaped organ containing thousands of delicate hair cells that convert sound vibrations into electrical signals, and the auditory nerve that carries these signals to your brain
Sound travels through each of these sections in sequence. A problem at any point along this pathway can result in hearing loss, but *where* the problem occurs determines what type of hearing loss you have.
What Is Conductive Hearing Loss?
Conductive hearing loss occurs when something prevents sound from being conducted efficiently through the outer or middle ear to the inner ear. Think of it as a physical barrier or mechanical problem that stops sound vibrations from reaching your cochlea at normal volume.
The key characteristic of conductive hearing loss is that your inner ear and auditory nerve typically remain healthy and intact. The problem lies in the delivery system, not the sensory organ itself. This distinction has enormous implications for treatment, as we’ll discuss shortly.
Common Causes of Conductive Hearing Loss
Conductive hearing loss can result from a range of conditions affecting the outer or middle ear:
Outer ear causes include earwax impaction (cerumen), foreign objects lodged in the ear canal, external ear infections (otitis externa), or narrowing of the ear canal (stenosis). These are often the simplest to identify and treat.
Middle ear causes tend to be more complex and may include middle ear infections (otitis media), fluid accumulation behind the eardrum (otitis media with effusion), eardrum perforation, dysfunction of the Eustachian tube, or problems with the ossicular chain. One particularly notable condition is otosclerosis, where abnormal bone growth around the stapes (the smallest of the three middle ear bones) prevents it from vibrating properly. Otosclerosis often develops gradually in adulthood and has a hereditary component.
The hallmark of conductive hearing loss is that it’s often temporary and can be medically or surgically treated. Removing impacted wax, treating an infection with antibiotics, placing ventilation tubes (grommets) for persistent fluid, or performing reconstructive middle ear surgery can frequently restore hearing to normal or near-normal levels.
What Is Sensorineural Hearing Loss?
Sensorineural hearing loss represents damage to the inner ear structures—particularly the cochlear hair cells—or to the auditory nerve pathways leading to the brain. According to Audiology Australia, this is the most common type of permanent hearing loss in adults.
Unlike conductive loss, sensorineural hearing loss affects your ear’s ability to convert sound vibrations into neural signals that your brain can interpret. Even if sound reaches your inner ear at an adequate volume, the damaged sensory system cannot process it correctly. This often results not just in reduced volume, but also in reduced clarity—patients frequently report that they can hear people talking but struggle to understand the words, particularly in noisy environments.
Common Causes of Sensorineural Hearing Loss
Sensorineural hearing loss stems from damage to delicate inner ear structures or neural pathways:
Age-related hearing loss (presbycusis) is the most prevalent cause, resulting from the natural degeneration of hair cells over time. This typically begins with high-frequency sounds and progresses gradually.
Noise exposure, whether from a single traumatic event (acoustic trauma) or years of cumulative exposure to loud environments, can permanently damage or destroy cochlear hair cells. This is increasingly common in younger populations due to recreational noise exposure.
Genetic factors can cause congenital hearing loss present from birth or progressive hearing loss that emerges later in life.
Medical conditions including Ménière’s disease, autoimmune inner ear disease, viral infections (such as measles, mumps, or cytomegalovirus), ototoxic medications (certain antibiotics, chemotherapy drugs, or high-dose aspirin), and head trauma can all damage the inner ear.
Sudden sensorineural hearing loss represents a medical emergency where hearing drops dramatically within 72 hours, requiring immediate evaluation and often corticosteroid treatment to maximise recovery chances.
The defining characteristic of sensorineural hearing loss is that it’s typically permanent. While we cannot regenerate damaged hair cells (unlike some animals that possess this remarkable ability), modern hearing aids and cochlear implants can effectively rehabilitate hearing function in most cases.
Mixed Hearing Loss: When Both Types Occur Together
Mixed hearing loss is exactly what it sounds like—a combination of both conductive and sensorineural components. A patient might have age-related sensorineural hearing loss that’s then compounded by a middle ear infection, or long-standing noise-induced damage with newly developed otosclerosis.
Understanding that mixed hearing loss has two separate components is crucial for treatment planning. The conductive portion may be medically or surgically reversible, potentially improving overall hearing even though the sensorineural component remains permanent. Your audiologist and ear, nose and throat (ENT) specialist will work together to determine the most appropriate management strategy.
How Audiologists Differentiate Between Types: The Power of Bone Conduction Testing
The cornerstone of differentiating conductive from sensorineural hearing loss is comprehensive audiometric testing that includes both air conduction and bone conduction measurements, as detailed in Stach’s *Comprehensive Dictionary of Audiology*.
Air conduction testing uses headphones or insert earphones to send sound through your entire hearing system—outer ear, middle ear, inner ear, and auditory nerve. This represents your overall hearing ability through the normal pathway.
Bone conduction testing uses a small vibrator placed on the bone behind your ear (mastoid process). This bypasses your outer and middle ear entirely, sending vibrations directly to your inner ear through skull bones. This isolated measurement tells us specifically how well your inner ear and auditory nerve are functioning.
The relationship between these two measurements is diagnostic:
When air conduction and bone conduction thresholds are similar and both show hearing loss, this indicates **sensorineural hearing loss**—the problem is in the inner ear or beyond.
When bone conduction thresholds are normal but air conduction shows hearing loss, this indicates **conductive hearing loss**—sound conducted through the air pathway is blocked, but when we bypass that pathway using bone conduction, hearing is normal.
When bone conduction shows some hearing loss and air conduction shows even greater loss, this indicates **mixed hearing loss**—there’s both an inner ear problem and a conductive component.
This difference between air and bone conduction thresholds is called the “air-bone gap,” and it quantifies the degree of conductive involvement. An audiogram will display this visually, making the distinction immediately apparent to trained clinicians.
Additional Diagnostic Tools
Beyond pure-tone audiometry, your audiologist may employ several additional assessments:
Tympanometry measures eardrum mobility and middle ear pressure, helping identify fluid, perforations, or ossicular problems. Acoustic reflex testing evaluates the middle ear muscle response to loud sounds. **Speech audiometry** assesses your ability to hear and understand words at various volumes. Otoacoustic emissions (OAEs) measure sounds generated by healthy outer hair cells in the cochlea—their absence suggests cochlear damage.
Together, these tools create a comprehensive diagnostic picture that guides appropriate intervention.
Treatment Implications: Why the Distinction Matters
The difference between conductive and sensorineural hearing loss fundamentally determines your treatment pathway.
Treating Conductive Hearing Loss
Because conductive hearing loss involves mechanical problems in otherwise healthy ears, medical or surgical intervention often provides excellent outcomes. Simple wax removal can immediately restore normal hearing. Antibiotics resolve many ear infections. Surgical procedures like tympanoplasty (eardrum repair), ossiculoplasty (middle ear bone reconstruction), or stapedectomy (for otosclerosis) frequently restore or significantly improve hearing.
When medical treatment isn’t appropriate or doesn’t fully resolve the hearing loss, hearing aids work exceptionally well for conductive losses because they simply need to provide additional amplification to overcome the conductive barrier—the sensory system remains intact to process the amplified sound clearly.
Treating Sensorineural Hearing Loss
Sensorineural hearing loss requires a different approach focused on compensation rather than cure. Hearing aids remain the primary intervention for mild to severe sensorineural hearing loss. Modern digital hearing aids don’t just make sounds louder—they selectively amplify frequencies where you have hearing loss, compress loud sounds to remain comfortable, reduce background noise, and can be precisely programmed to your unique audiometric configuration using real-ear measurement (REM) to verify appropriate amplification.
For severe to profound sensorineural hearing loss where hearing aids provide insufficient benefit, cochlear implants bypass damaged hair cells entirely by directly stimulating the auditory nerve with electrical signals. These remarkable devices have transformed outcomes for profoundly deaf individuals.
Assistive listening devices, communication strategies, and auditory rehabilitation can further enhance your ability to function effectively in challenging listening situations.
Treating Mixed Hearing Loss
Mixed hearing loss may benefit from addressing the conductive component first—perhaps through medical treatment or surgery—before optimising hearing aid fitting for the remaining sensorineural component. This staged approach often provides the best overall outcome.
When to Seek Professional Evaluation
You should arrange a comprehensive hearing assessment with a qualified audiologist if you experience:
– Gradual difficulty hearing conversations, particularly in background noise
– Frequently asking people to repeat themselves
– Turning up television or radio volume beyond what others find comfortable
– Sudden hearing loss in one or both ears (seek urgent evaluation)
– Persistent ear fullness, pressure, or pain
– Hearing loss accompanied by dizziness or tinnitus (ringing in the ears)
Certain “red flag” symptoms warrant urgent medical evaluation, including sudden hearing loss, hearing loss in only one ear, hearing loss accompanied by severe dizziness or neurological symptoms, or hearing loss following head trauma.
Understanding the difference between conductive and sensorineural hearing loss empowers you to have informed conversations with your healthcare providers and make appropriate decisions about your hearing care. Conductive hearing loss, arising from outer or middle ear problems, is often medically treatable and sometimes completely reversible. Sensorineural hearing loss, resulting from inner ear or nerve damage, is typically permanent but highly manageable with appropriate amplification and rehabilitation. Mixed hearing loss combines elements of both.
The good news is that regardless of which type of hearing loss you have, effective interventions exist. Modern diagnostic techniques allow audiologists to precisely identify the nature and degree of your hearing loss, enabling targeted treatment that can significantly improve your quality of life, communication ability, and social engagement.




{kind=link}
{kind=link}
{kind=link}