
Ear pain has a way of stopping life in its tracks. It interrupts sleep, derails work or school, and often arrives with a blend of muffled hearing, pressure, and worry. Part of the confusion stems from the fact that “ear infection” is an umbrella term that encompasses a wide range of different problems.
At The Audiology Place in Forestville, we dedicate a significant amount of time to helping families distinguish between two of the most common conditions: otitis externa, commonly referred to as swimmer’s ear, and otitis media, a middle ear infection. Knowing which one you’re dealing with matters because the cause, treatment, and follow-up are not the same.
Before we separate the two, it helps to picture where they occur. The outer ear canal is the narrow corridor you can’t quite see into, a delicate sleeve of skin that runs from the bowl of your ear (the concha bowl) to the eardrum. That’s where otitis externa sets up camp—on the skin itself. The middle ear, by contrast, is an air-filled cavity behind the eardrum that connects to the back of your nose via the Eustachian tube. When this space becomes inflamed or filled with fluid, it is known as otitis media: same ear, different neighbourhoods.
Otitis externa tends to announce itself with irritation and tenderness right at the entrance. Patients often describe an itchy, sore feeling that becomes distinctly worse when the outer ear is touched or gently tugged, as if the skin itself is bruised. Because the ear canal is remarkably effective at trapping whatever we put in it, moisture is the classic trigger. Days at the pool, ocean swims, long, steamy showers, or even just Sydney’s humid weather can soften the canal skin and alter its pH, inviting bacteria or fungi to flourish. Cotton tips and improvised “cleaning” tools exacerbate the issue by micro-scratching the skin and pushing wax or other debris deeper. A thin, watery or slightly cloudy discharge is common, as is a temporary blocked sensation as swelling narrows the canal; hearing can feel dulled for a few days simply because sound has to squeeze past inflamed tissue.
Self-care for this outer-ear problem is refreshingly practical, provided no red flags are present. The rule of thumb is to keep the canal dry and undisturbed while the skin heals. This means avoiding further prodding with cotton tips, resisting home remedies that coat or clog the canal, and protecting the ear while showering. Where an audiologist or GP has confirmed that the eardrum is intact, short courses of specific over-the-counter drying or acetic solutions can help normalise the canal’s environment. If pain escalates, the skin around the ear becomes increasingly red and swollen, or symptoms linger beyond a couple of days, it’s time for hands-on care and likely prescription drops from your GP. Untreated otitis externa can become persistent, and in individuals with diabetes or weakened immunity, it warrants prompt medical attention.
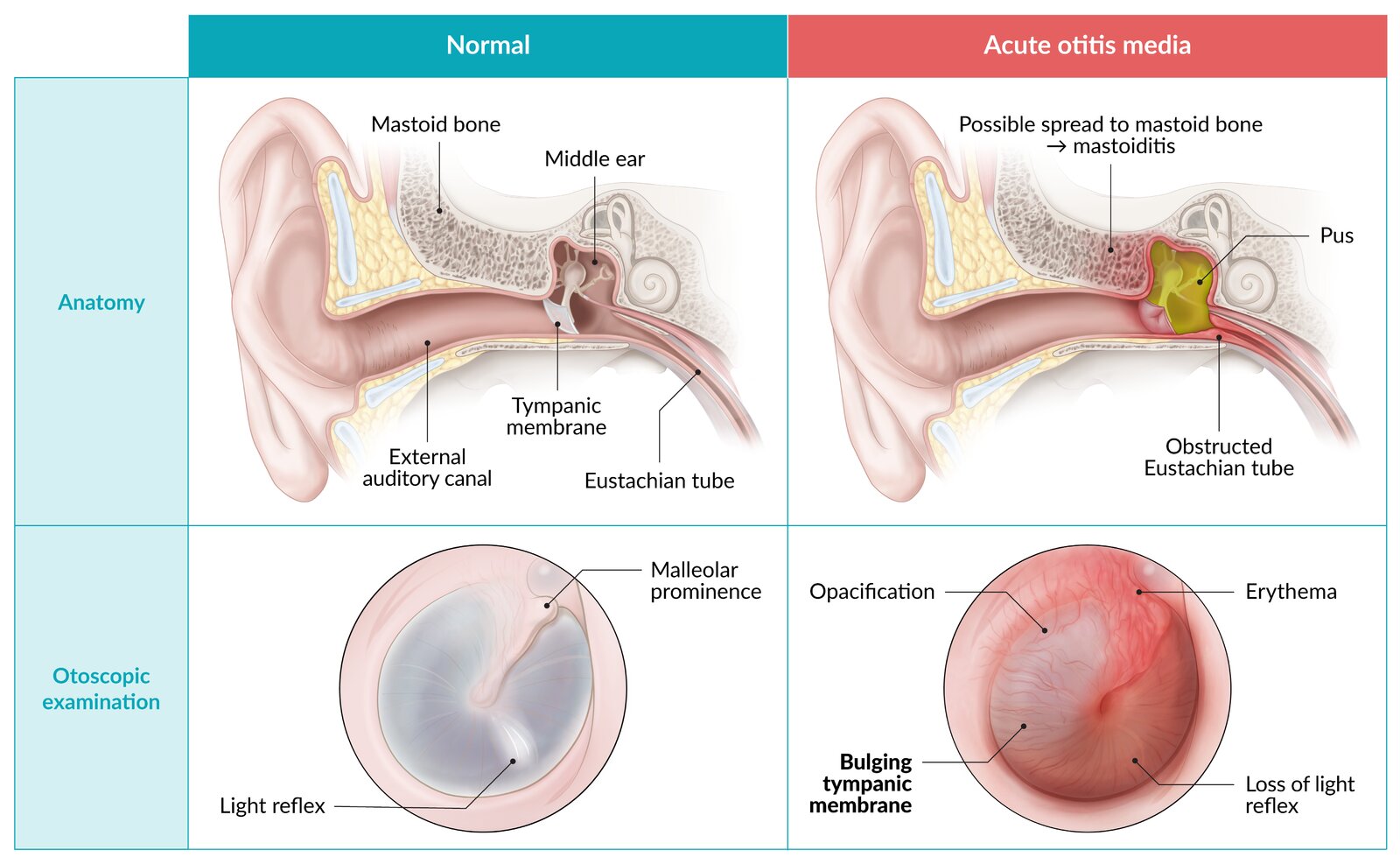
https://www.amboss.com/us/knowledge/acute-otitis-media
Otitis media, by contrast, lives behind the eardrum and often arrives on the coattails of a cold or a bout of hay fever. In children—especially under five—it’s extraordinarily common because their Eustachian tubes are more horizontal and easily blocked, trapping air and fluid in the middle ear. Adults aren’t immune, but we’re more likely to notice it as a heavy, pressure-like pain that worsens when we lie down, accompanied by muffled hearing and a sense of fullness. Fever is more likely here than with swimmer’s ear, particularly in younger children, who may also be irritable or lose their appetite. Sometimes, if pressure becomes high enough, the eardrum can perforate, releasing thick fluid into the canal. The sudden drainage can appear dramatic, but many people experience immediate pain relief as the pressure is relieved; the eardrum generally heals, although medical follow-up is essential.
Supportive care during those first forty-eight hours often focuses on comfort, including appropriate pain relief, adequate hydration, rest, and sensible monitoring. Because a proportion of acute middle ear infections are viral, antibiotics are not always the first step; your GP will weigh up age, severity, duration, and examination findings. What matters for families is to watch the trajectory. A steadily improving child with manageable discomfort is very different to a miserable child whose pain and fever remain high at the three-day mark. Adults should take the same approach: if pain is severe, hearing is rapidly deteriorating, or symptoms persist or worsen after a couple of days, a medical assessment is the right move.
Several red flags should trigger immediate care, regardless of which type of ear infection you suspect. High fevers (above 39 °C), spreading redness or swelling around the ear, persistent dizziness or spinning sensations, any new facial weakness, sudden hearing loss, or foul-smelling/bloody drainage are all warning signs that something more complex may be happening. People with diabetes, those who are immunocompromised, or anyone with a recent head injury should be cautious and seek help early. It’s always better to check than to wait and worry.
Prevention unsurprisingly mirrors the mechanics of each condition. For swimmer’s ear, water management is king. Many of our Northern Beaches patients thrive with a simple routine after surf or pool sessions: gently tilt and towel the outer ear, avoid inserting anything into the canal, and consider well-fitting swim plugs if you’re prone to flare-ups. Maintaining the canal’s natural balance—rather than trying to “sterilise” or “de-wax” it—is the goal; your ears have their own housekeeping system, and over-cleaning destabilises it.
For middle ear problems, the focus shifts to upper-airway health. Good hand hygiene, up-to-date vaccinations according to GP guidance, allergy management, and a smoke- and pollution-free environment all reduce the background conditions that lead to Eustachian tubes clogging and the middle ear filling. In children with frequent infections, your GP or an ENT specialist may discuss the role of adenoids, tonsils, and other anatomical contributors.
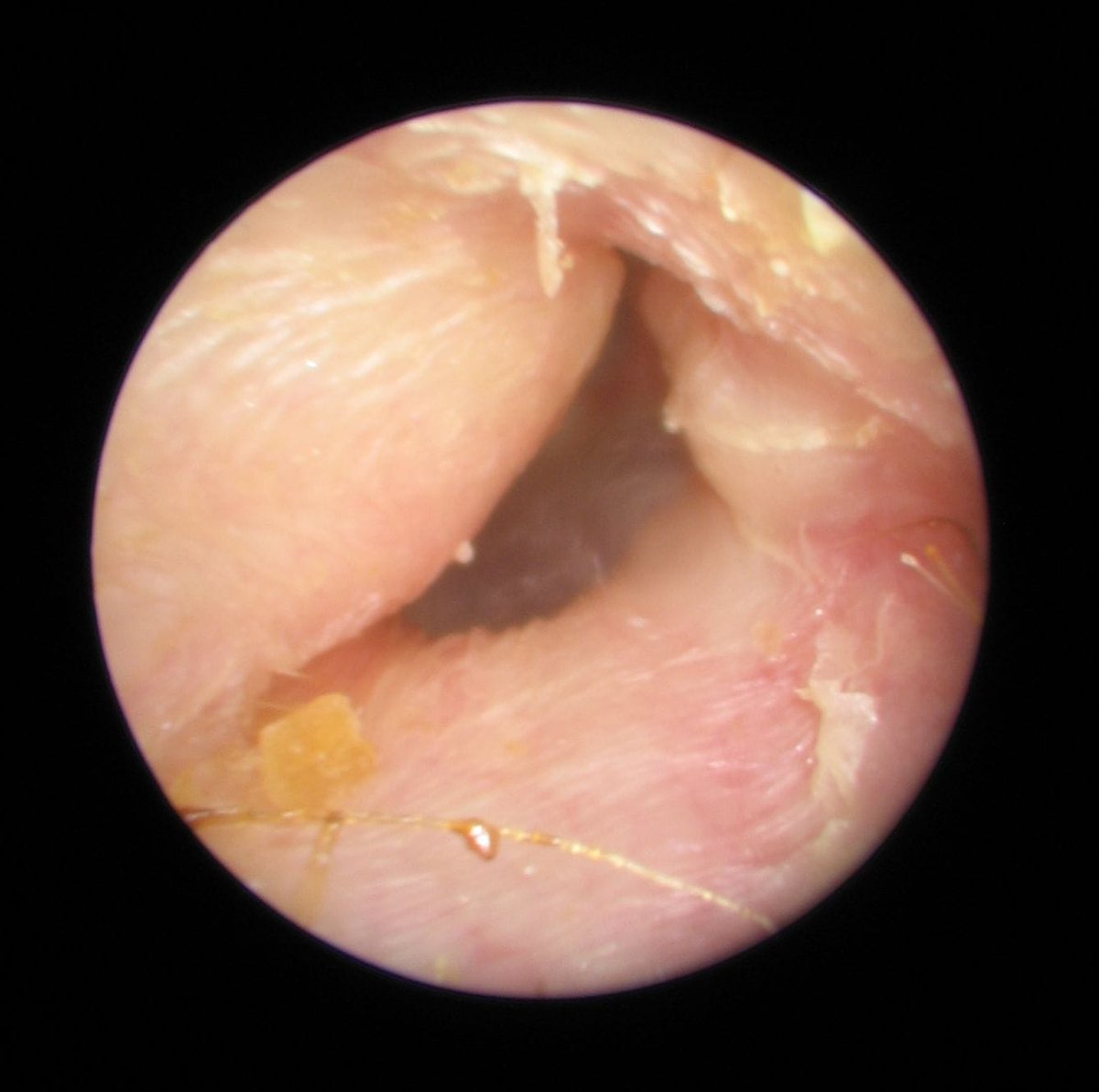
Where does an audiology clinic fit into all of this? At The Audiology Place, we begin with a thorough case history and then utilise tools that provide accurate insights, rather than relying on guesswork. Video otoscopy lets us share a clear image of the ear canal and eardrum on screen, so you can literally see the difference between a swollen, debris-lined canal and an angry, bulging eardrum. Tympanometry measures how well the eardrum moves and whether negative pressure or fluid is present behind it—a quick, painless test that’s invaluable for sorting out middle ear issues. Age-appropriate hearing tests add context: even temporary conductive changes in children can affect listening effort and classroom attention, so it’s helpful to know how much sound is actually getting through. When wax is the culprit—or when a clear view of the eardrum is needed to assess the condition—gentle microsuction can be performed to remove the blockage safely. From there, we’ll provide a plain-English summary you can share with your GP, along with any images and tympanometry results to inform treatment decisions.
It’s also helpful to draw a line between diagnosing infections and optimising hearing. Real-Ear Measurement (REM), which you’ll see mentioned across our site, is the gold-standard verification step we use when fitting hearing aids; it ensures the sound reaching your eardrum matches the prescription for your hearing loss. REM is not used to diagnose otitis externa or otitis media. However, if a middle ear problem has temporarily reduced hearing in a hearing aid user, or if infections have been part of a more extended history of fluctuating thresholds, we’ll use verification later to ensure any amplification is precise and comfortable once the ear is healthy again.
Follow-up matters more than people think, particularly for children. A child who has pushed through a nasty middle ear infection can feel “back to normal,” yet still have lingering fluid that softens consonants and makes listening in class strangely tiring. Scheduling a brief review to confirm that the middle ear has returned to normal pressure and that hearing has returned to baseline is a small step with significant educational benefits. For adults, the same principle applies: if an infection coincides with a noticeable decline in hearing or persistent tinnitus, a re-check is worthwhile. And if we’ve referred you to your GP or an ENT, we’ll ensure your medical practitioner receives our notes, so your care remains coordinated.
Living on the Northern Beaches, we naturally see many people who love the water. We also know the frustration that comes from avoidable setbacks, such as cotton tips that seemed like a good idea or a busy week that pushed off a needed review. The good news is that most outer and middle ear problems respond quickly to the right plan. Keep canals dry and unprodded when the skin is angry. Respect the middle ear’s tendency to follow the nose—treat the cold, support the Eustachian tube, and be patient as pressure equalises. Watch the pattern over forty-eight to seventy-two hours and don’t ignore red flags. And when in doubt, let us take a look: a photo of your eardrum and a tympanometry trace can save a week of guesswork.
If you or your child is experiencing ear pain, blocked ears, recurrent infections, or a combination of symptoms, we’d be happy to help. Our clinic in Forestville offers calm and thorough assessments for adults and children, with same-day appointments available when possible. You’ll leave with answers you can see, a plan you can follow, and clear guidance on when to consult your GP or an ENT specialist.
This article provides general information and is not a substitute for medical advice. Always seek the guidance of your GP for diagnosis and treatment, and call 000 in an emergency.
References
Bhutta, M. F., Leach, A. J., & Brennan-Jones, C. G. (2024). Chronic suppurative otitis media. The Lancet, 403(10441), 2339-2348.
Ellis, J., De La Lis, A., Rosen, E., Simpson, M. T., Beyea, M. M., & Beyea, J. A. (2024). Approach to otitis externa. Canadian Family Physician, 70(10), 617-623.
Gupta, A. (2021). The Discharging Ear: Differential Diagnosis and Management. In Manual of Contemporary Otological Practice (pp. 76-96). CRC Press.
Jackson, E. A., & Geer, K. (2023). Acute otitis externa: rapid evidence review. American family physician, 107(2), 145-151.
Sideris, G., Petsiou, D. P., Kourklidou, M., Papadimitriou, N., Vlastarakos, P. V., Karamagkiolas, S., … & Delides, A. (2024). Fungal malignant otitis externa: a systematic review. Cureus, 16(10).
Jamal, A., Alsabea, A., Tarakmeh, M., & Safar, A. (2022). Etiology, diagnosis, complications, and management of acute otitis media in children. Cureus, 14(8).
Merchant, G. R., Al-Salim, S., Tempero, R. M., Fitzpatrick, D., & Neely, S. T. (2021). Improving the differential diagnosis of otitis media with effusion using wideband acoustic immittance. Ear and hearing, 42(5), 1183-1194.
Sirota, S. B., Doxey, M. C., Dominguez, R. M. V., Bender, R. G., Vongpradith, A., Albertson, S. B., … & Ed-Dra, A. (2025). Global, regional, and national burden of upper respiratory infections and otitis media, 1990–2021: a systematic analysis from the Global Burden of Disease Study 2021. The Lancet Infectious Diseases, 25(1), 36-51.




{kind=link}
{kind=link}
{kind=link}