 - The Audiology Place")
How one patient found answers, validation, and a path forward
Sarah’s Story
Sarah* is 34 years old and works in government administration. For as long as she can remember, certain sounds have made her feel like she was losing control. As a child, she noticed that the way her family members chewed food or cleared their throats would send her into a spiral of irritation she couldn’t explain. She thought she was just “oversensitive.” Her parents thought the same.
The problem got worse. Much worse.
By her mid-twenties, Sarah found herself constantly asking her husband and mother to stop making certain sounds. Chewing. Crunching. Slurping. Sniffing. These weren’t loud noises that would bother anyone. They were quiet, everyday sounds that most people filter out without thinking. For Sarah, they triggered an instant flood of anger and agitation that could take hours to shake off.
Then new triggers appeared. Her husband’s breathing at night started to bother her. The anticipation of hearing a trigger sound became almost as distressing as the sound itself. She would walk into a room already tense, already bracing herself for what she might hear. She wasn’t just reacting to sounds anymore. She was living in a constant state of alert.
The guilt was crushing. Here was a woman who genuinely loved her husband and mother, and yet she found herself snapping at them, asking them to change perfectly normal behaviours. She felt embarrassed about her reactions. She worried that explaining her triggers would make her seem difficult or demanding. She felt isolated in a problem no one around her seemed to understand.
Finding Out What It Actually Was
Sarah had experienced significant anxiety about 18 months before coming to see us. She’d worked through that with her doctor, and the anxiety had improved. But the sound sensitivity hadn’t budged. If anything, it had intensified. She’d tried deep breathing when triggers occurred, but that just left her exhausted from the effort of trying to suppress her reactions.
What Sarah didn’t know was that her anxiety and her sound sensitivity weren’t the same thing. Treating one hadn’t touched the other because they operate through different pathways in the brain. This is one of the most common misunderstandings about misophonia. People assume it’s a psychological problem, something you can think your way out of, or meditate away, or simply choose to stop. It’s not.
When Sarah came to The Audiology Place for a misophonia assessment, she scored 44 on the Misophonia Assessment Questionnaire. Anything above 40 indicates severe misophonia. Her responses on the Misophonia and Hyperacusis Questionnaire confirmed severe misophonia but showed hyperacusis was unlikely. Her DASS-21 results painted an interesting picture: depression and anxiety scores were minimal (1 and 1), but her stress score was elevated at 8.
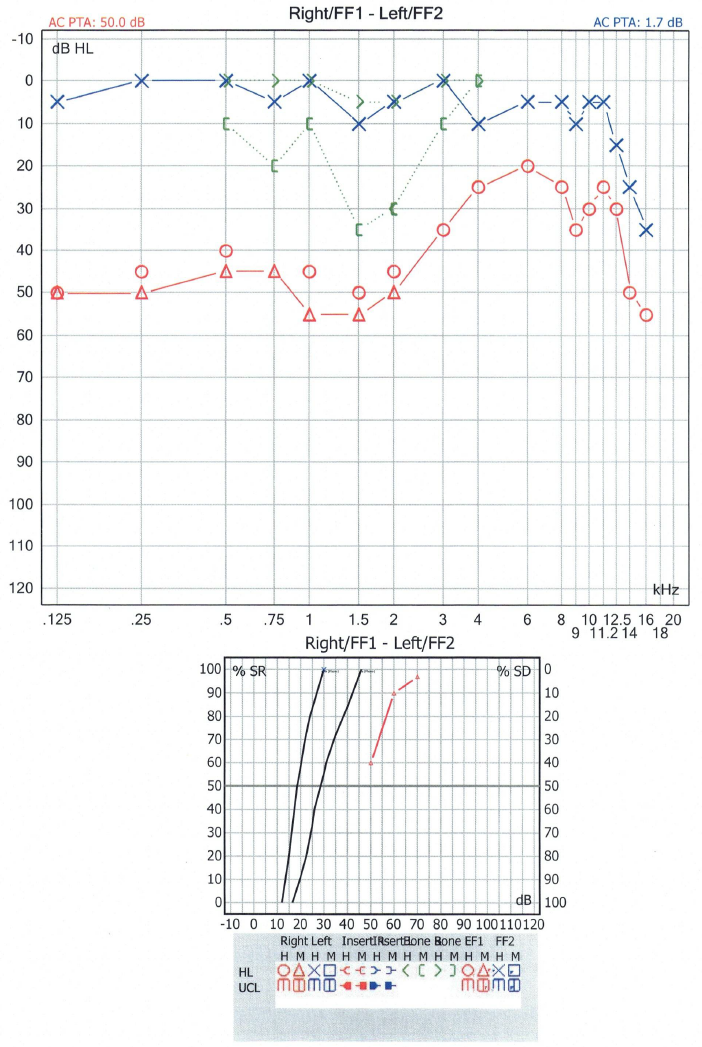
We ran a full audiological workup. Her hearing was excellent across the entire frequency range, from 250Hz all the way up to 16,000Hz in the extended high frequencies. Some of her thresholds actually fell below 0dB, indicating heightened sensitivity. Tympanometry showed healthy middle ear function bilaterally. We skipped acoustic reflex testing because presenting loud sounds to someone in the middle of a misophonia assessment would be unnecessarily distressing. Otoacoustic emission testing was well tolerated and indicated health outer hair cell function in Sarah’s inner ears.
Her Uncomfortable Loudness Levels came back normal. This was important. Hyperacusis involves discomfort from sound intensity. Misophonia is triggered by specific sound patterns regardless of how loud they are. The tap of a finger. The click of a tongue. The soft sound of someone breathing through their nose. Sarah’s ears were working perfectly. Her brain’s association with certain sounds was the problem.
What’s Going On in the Misophonic Brain
We spent a good portion of our session explaining what’s happening neurologically. Most people with misophonia have never heard a clear explanation of why their brain does this. Understanding the mechanism doesn’t make the triggers disappear, but it changes everything about how you relate to the condition.
Picture your brain’s auditory system as a sophisticated filtering operation. Every second, your ears pick up hundreds of sounds. Most of them get filtered out before they reach conscious awareness. The hum of your refrigerator. Traffic noise outside. Your own breathing. You don’t notice these because your brain has decided they’re not important.
In misophonia, certain sounds skip the filter entirely and go straight to the threat detection system. The anterior insular cortex, which normally helps us assign emotional meaning to sensory input, lights up like a Christmas tree. Your brain treats the sound of someone chewing with the same urgency it would treat footsteps behind you on a dark street. Fight or flight kicks in. Adrenaline floods your system. Your muscles tense. Your heart rate spikes. All because someone took a bite of their sandwich.
Sarah also showed signs of misokinesia, the visual counterpart to misophonia. Just the thought of a trigger sound occurring, or seeing someone’s jaw move before they chew, could set off her stress response. This meant her brain had learned to anticipate threats, not just react to them. She was essentially living in a state of constant vigilance.
Building a Path Forward
Misophonia treatment isn’t about curing the condition overnight. It’s about changing the relationship between your brain and these trigger sounds over time. We put together a multi-pronged approach for Sarah that addressed different aspects of her experience.
Sound therapy/sound enrichment therapy through bone conduction headphones became Sarah’s first line of defence. Devices like Shokz headphones deliver white noise directly through the bones of the skull, allowing all ambient sounds (including triggers) to enter through the normal ear canal pathway. The white noise creates a kind of acoustic cushion. The triggers still arrive at Sarah’s brain, but they land on a softer surface. Over time, this helps the brain learn and rewire that these sounds don’t warrant a threat response.
Loop earplugs offer an interim solution for severely triggering environments or situations. These aren’t the foam plugs you’d use at a construction site. Loop earplugs (specifically the “Quiet” model) offer 24dB of sound reduction while preserving speech frequencies. This means Sarah can still follow conversations but with a comfortable “blanket” of attenuation over the sharpness of her triggers. We talked about the importance of not overusing them. Complete sound avoidance can actually make misophonia worse because your brain becomes even more sensitized when it hasn’t heard background noise for a while. When we utilise sound deprivation, it is reinforcing to the brain that “quiet is safe, and noises are a threat”.
Psychological support rounds out the approach. We referred Sarah to MindBox Psychology in St Leonards, where clinical psychologists specialise in misophonia using Cognitive Behavioural Therapy and Acceptance and Commitment Therapy. These aren’t about teaching you to “just relax” or think positive thoughts. They’re about building genuine psychological flexibility, finding ways to coexist with your triggers rather than being controlled by them.
We also prescribed something often overlooked:
dedicated relaxation time. Sarah’s nervous system was operating in high gear most of the day. The constant vigilance, the suppression of reactions, the effort of managing her emotional responses. All of that takes a toll. Regular, deliberate downtime where she can actually let her guard down isn’t a luxury. It’s part of the treatment. Knowing through hard periods of the day, that you will have your safe, quiet, regulation time at the end of the day, can soften the anxiety that so often comes with “holding in” what we are feeling.
What a Diagnosis Actually Means
When we told Sarah she had severe misophonia, something shifted in the room. Relief. She wasn’t broken. She wasn’t dramatic. She wasn’t “too sensitive.” She had a recognised neurological condition with a name, a body of research behind it, and treatment options that actually address the underlying mechanisms.
We talked about how to explain misophonia to her family. This is often one of the hardest parts. It’s one thing to understand your own condition. It’s another to help the people you love understand why certain sounds affect you the way they do, and to ask for accommodations without feeling like a burden.
The key message we gave Sarah to share with her husband and mother: this isn’t about the sounds being “too loud” or Sarah being “too fussy.” Her brain processes these specific sounds differently at a neurological level. She can’t control the initial reaction any more than you can control flinching when someone pretends to throw something at your face. What she can control, with support and treatment, is what happens after that initial reaction.
The Good News About Neuroplasticity
Here’s the thing about brains: they change. The same neuroplasticity that allowed Sarah’s misophonia to worsen over time, with new triggers emerging and anticipatory anxiety developing, can work in the other direction. The brain learned to treat these sounds as threats. It can learn to treat them differently.
This doesn’t happen quickly. We’re talking months of consistent work with sound therapy, psychological support, and practical coping strategies. But it does happen. The trigger sounds don’t necessarily stop being noticeable. They stop being unbearable. The fight-or-flight response becomes less intense. The recovery time shortens. The anticipatory anxiety loosens its grip.
Sarah left our clinic with a clear diagnosis, a treatment plan, referrals to the right specialists, and something she hadn’t had in years: hope. She now understood what she was dealing with. She knew it was real. And she knew there was a way forward.
Does This Sound Familiar?
If you’re reading Sarah’s story and recognising yourself in it, please know that you don’t have to keep struggling in silence. Misophonia is real. It’s measurable. And it’s treatable. And our Audiologist Dr. Signe Steers understands this first hand.
At The Audiology Place in Forestville, we conduct comprehensive misophonia assessments that include validated questionnaires, full audiological testing, and education about what’s happening in your brain. As an independent clinic, we’re not tied to any particular product or treatment approach. We build a management plan around what you specifically need.
If you’ve been living with sound sensitivity that affects your relationships, your work, or your quality of life, book an appointment. Let’s find out what’s going on and build a path forward together.
Book your misophonia assessment: Call (02) 9315 8327 or visit theaudiologyplace.com.au
*Name changed to protect patient privacy. Case details shared with patient consent.


{kind=link}